The Ultimate Hair Loss Survival Guide For Men (FAQ)
Originally written by xRedStaRx from bb.com/misc
This is a comprehensive guide gathering all of the relevant and scientifically backed up information with regards to hair loss, and featuring the most frequently asked questions that usually come up. The goal of this thread would be guiding people who would like to do something about their hair, but unable unable to conduct proper research, free of unscientific bias. In retrospect of the previous hair loss thread, I do not encourage you to flood my inbox with private messages, any further questions beyond the scope of this thread should be posted here, publicly. There are many people on this board just as knowledgeable as I am with hair loss and their treatments, and hopefully even more so, that should provide you with a better perspective overall than otherwise.
Please refrain from posting previously answered questions, use the search function if possible, any redundant questions may not be answered. Do not attempt posts convincing people to shave their heads, this is not the proper thread for such. I've already outlined this type of questions in the FAQ, and any further discussions should be done in a separate thread. Most of the questions and their subsequent answers in this FAQ come from either the previous thread, or questions I've personally received through PM. Go through them carefully if you need to, any inquiries you may have is most likely included. If you are not losing your hair, or indifferent towards them, it will most likely be a complete waste of time to go through this thread, but whatever you choose to do, please do not waste time and space for others who seek help.
Before I start, please note the following: I am not a physician, I do not promote nor condone the use of treatments or medication without professional medical supervision if necessary. I will not be held liable under any event, let that be positive or negative, from the improper use of information in this thread. I will be mostly stating facts and figures based on thorough research from peer-reviewed journals, publications and clinical trials done on human and animal models. The decision and subsequent responsibility, remains completely yours.
Good, let's begin.
1. Overview
1.1 What is androgenic alopecia?
Everyone has some degree of MPB, all males have hair follicles on the vertex and front of their scalps that's sensitive to androgens. But the amount of sensitivity, tissue expression, and androgen levels give us all different ranges and patterns for MPB. People need to understand that hairloss is genetic. No amount of diet, lifestyle, or shampoos will save it. If your genetic makeup writes off your hair, then you are fighting a losing battle. Genetic differences between subjects, such as polymorphisms in 5α-reductase, may also contribute to the intersubject variability, and hence, receptibility to treatment and susceptibility to hair loss. Now getting to the bottom of why MPB happens to some people, while others who have high amounts of scalp DHT with no hair loss, is still under study. So far, the most recent findings on the path to curing hair loss seems to pinpoint Prostaglandin D2, known as PGD2 and its derivative, 15-dPGJ2, as one of the main culprits for AGA.
We show that prostaglandin D(2) synthase (PTGDS) is elevated at the mRNA and protein levels in bald scalp compared to haired scalp of men with AGA. The product of PTGDS enzyme activity, prostaglandin D(2) (PGD(2)), is similarly elevated in bald scalp. During normal follicle cycling in mice, Ptgds and PGD(2) levels increase immediately preceding the regression phase, suggesting an inhibitory effect on hair growth. We show that PGD(2) inhibits hair growth in explanted human hair follicles and when applied topically to mice. Hair growth inhibition requires the PGD(2) receptor G protein (heterotrimeric guanine nucleotide)-coupled receptor 44 (GPR44), but not the PGD(2) receptor 1 (PTGDR). Furthermore, we find that a transgenic mouse, K14-Ptgs2, which targets prostaglandin-endoperoxide synthase 2 expression to the skin, demonstrates elevated levels of PGD(2) in the skin and develops alopecia, follicular miniaturization, and sebaceous gland hyperplasia, which are all hallmarks of human AGA. These results define PGD(2) as an inhibitor of hair growth in AGA and suggest the PGD(2)-GPR44 pathway as a potential target for treatment. One would think that people genetically predisposed to MPB somehow undergo increased PGD2 pathway activity in their balding scalps through an unknown mechanism, most likely triggered through DHT production, since we all know DHT is the first variable of the AGA equation. An elimination of PGD2 expression in scalp tissue should help with hair loss in this case. The mechanism for losing hair is definitely not simple. It's all related, one way or another, to your specific hormonal and AR profile, and genetics. Look at this chart.
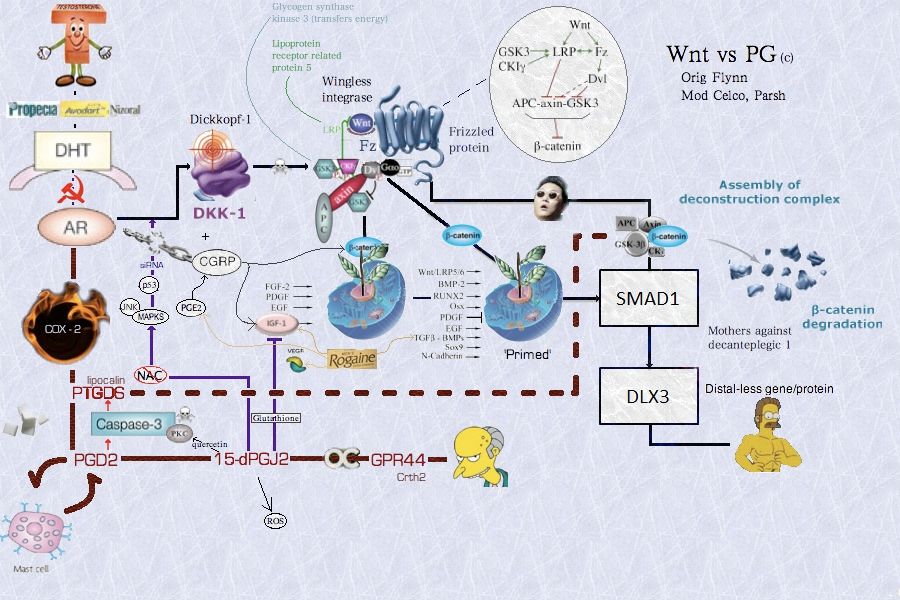
This goes to show the immense amount of factors coupled that lead to hair loss. There's a reason why 5AR inhibitors stop and reverse hair loss. Literally interfering with any of these pathways or protein codings would help with hair loss, it's also interesting to point out from this chart why Finasteride and Dutasteride are so effective at preventing hair loss, which is also parallel to the model of why pseudohermaphrodites with congenital 5-Alpha-Reductase II deficiencies keep a youthful head of hair throughout their lives. Because it eliminates the mother of all these pathways, DHT. Cut that out of the equation, and you'd experience severe depression in DKK-1 and COX-2 pathways, both which have metabolites proven to exist in high numbers and very active forms on bald scalps. The specificities on the mechanism of how it stops hair from growing is still speculation at this point, but we do have a very good general idea of how they all add up. For example, finasteride has also been shown to work best on people who have high IGF-1 levels, whether or not the effect is direct is not fully known, but keep in mind that DKK-1 activity represses IGF-1 production, so IGF-1 levels may not have a direct effect on hair follicles, but it is simply a marker for weak DKK-1 expression. If we can somehow inhibit the cyclooxygenase-2 enzymes or the PTGS2 gene on one hand, and depress the pathway activity of DKK-1 gene on the other, all in one effective method of treatment, then we can skip the process of inhibiting 5-AR enzymes all together.
1.2 Why do most men lose their hair?
As in regards to where baldness comes from, I wish it was that easy, genetics is like rolling dice, depending on the chromosomes you inherit from each parent, create your genetic makeup and their respective expressions. The maternal lineage seems to be slightly more responsible for MPB, since one of the key factors in it, which is AR sensitivity, is only coded on the X chromosome.
Big scale studies in 2005 and 2007 emphasize the significance of the maternal line in the inheritance of male pattern baldness and have decided that male pattern baldness is hereditary passed down on the mother's side. The explanation is genetic and linked to your mother's X-Chromosome. Premature male pattern baldness has something to do with the sex chromosomes, to be accurate, the X chromosome, which a man inherits from his mother. Each person gets one-half of their genetic make-up from their mother and the other half from their father. There are two chromosomes, X and Y. Each person has a set of two chromosomes: males are XY and females are XX. When a child is conceived, the mother contributes an X chromosome, and the father contributes either the X chromosome or the Y chromosome. It is the X chromosome that contains the gene for male pattern baldness. A certain variant of the androgen receptor (AR) gene, on the X chromosome, is needed for androgenetic alopecia (AGA), or premature male pattern baldness, to progress. This specific gene is recessive, and the female would need to have both X chromosomes with the variant, or else she would pass on the dominant gene which would preclude male baldness.
On the other hand, another study shows that it's much more complex than that. It seems family history from the paternal lineage has statistically larger significance.
The heterogeneity in the clinical phenotype further suggests that AGA is inherited as a complex trait disorder. It's reported in one of the studies that 81.5% of bald Caucasian sons had bald Caucasian fathers. The "baldness gene" (assuming this is true for simplicity) comes from both parents, and is additive, not recessive or dominant. What this means is, depending on the count of family members on both sides of your family who have gone bald, this is your odds of going bald as well. If 5/6 uncles (including your dad) and grandfathers on your paternal side are bald, and 2/3 of your uncles and grandfathers on your maternal side are bald, then odds that you will go bald is roughly (5+6)/(6+3)= 78%. It's not what exactly happens on a genetic level, but it's an easy and approximate method to find out the likelihood for your hair condition. The more family members you have, the lower the margin of error.
1.3. Am I balding?
Miniaturization may be the best way to identify androgenic hair loss. Do you have thinner and shorter hairs all over the edge of the hairline? Only 15% of all hair is in telogen phase at any given time, if you do have a lot of weak hair on the hairline that's in a telogen phase (thin and shorter hair), then you probably have MPB. It will take about a year or two for these hairs to stop growing completely, and whether or not the hair follicles behind them will have tissue expression that let's them suffer the same consequences might still be too early to tell. If you cannot see any miniaturization, then your hair loss isn't likely androgenic. Shedding might be from AA or Telogen effluvium. Check for Hypogonadism or Hypothyroidism. Every male gets a receding hairline, the severity of it gets classified as either a NW1 or a NW2, both are not considered male pattern baldness. But you cannot maintain a NW0 for life. Generally, anything beyond NW2 is officially MPB.

2. Treatments
2.1 Do treatments work?
Only a minority do, the only treatments proven to work are listed here. Supplements, shampoos, vitamins, minerals, laser therapy, all of these are controversial at best. And have no solid basis in medical literature. I'm personally not a big believer in natural oils and remedies. The results seem inconsistent and there isn't enough clinical trials done this matter to assess it's efficacy in terms of hair counts. Treatments, with whatever you choose, should be a life time commitment. Any changes in regimen triggers hair sheds. You should construct a regimen you are comfortable with and stick to it for best results. The following treatments do work for AGA, so read and learn carefully about each one and how they all fit together.
2.2 How long until I see results?
Normally, it takes quite a while to see any decent results. A typical timeframe would be shedding and slowing down of hair loss from 0-3 months, hair loss halting or improving starting from 3-6 months, some visible regrowth from 6-9 months, and the final saturated hair condition on the 12-24 month mark. Some treatments work faster than others. For example, ketoconazole and minoxidil typically show results faster than all the others. So don't feel pressured, a follicle can be dormant for three months before growing out again, be patient until the very end before deciding whether they are working for you or not.
2.3 What treatments can I use?
2.3.1 5-Alpha-Reductase inhibitors
2.3.1a Finasteride
The government should be sprinkling finasteride on every male's cereal bowl past 18 years old. Not srs. Some of you may know finasteride by it's trade name, propecia. Finasteride is neither a hormone nor a derivative of it, it is simply a very potent suicide inhibitor of 5-AR II and III enzymes. It has been FDA approved since 1991, and has other uses besides hair loss. Finasteride can potentially work on all hairs of the scalp, although it tends to have better results on the vertex and mid-anterior parts, as opposed to the frontotemporal regions.
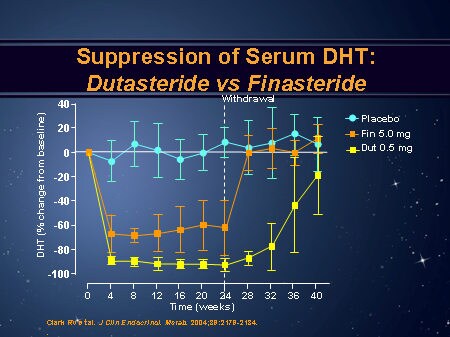
Now pharmacology tells us that only 0.05mg of finasteride was almost 50% as effective as 100 times the dose of 5mg in reducing serum DHT after a single dose.
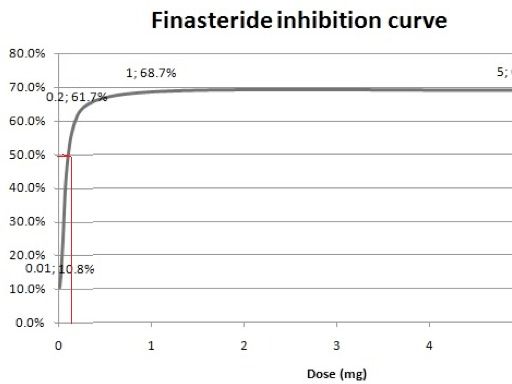
Not only that, but 0.05mg was close to 90% as effective after daily dosing in reducing serum DHT. Look at the following study:
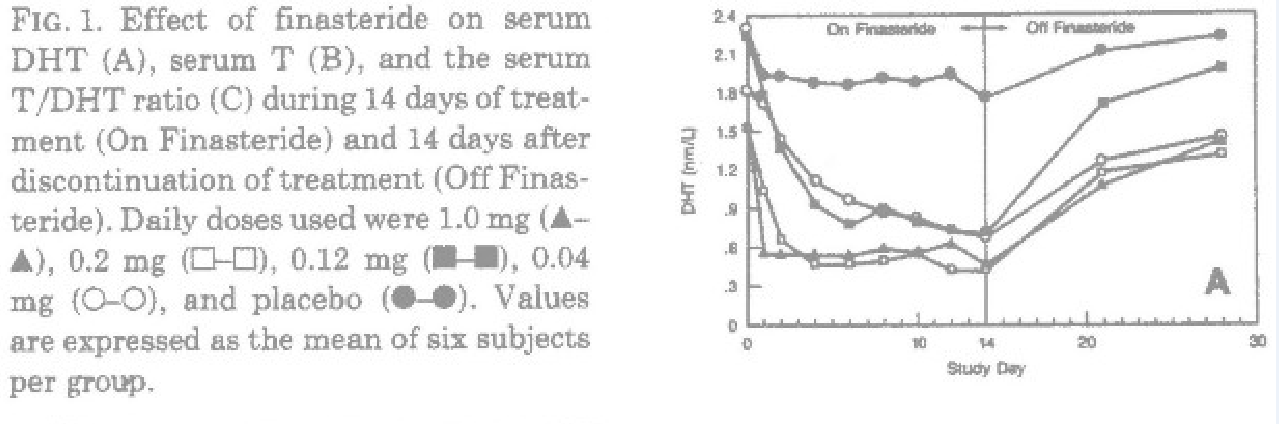
It takes about 4 days of everyday usage to achieve a steady-state concentration of finasteride in serum levels. Finasteride begins to achieve close to 90% of it's maximal efficacy after a single oral dose above and including 0.5mg. 0.2mg/day was the least optimal dose to get the same response as a full 1mg dose, in reducing serum DHT. In other words, 1.4mg/week works almost as well as 7mg/week in reducing serum DHT.
The general consensus on the 1mg dose has to do with the early MERCK trial in 1998 before propecia hit the markets. Where it showed that this dose provided the best compensation for hair growth and amount of dosage, according the logarithmic dose-response curve getting flat close to 1mg. We will see later on that serum DHT levels and subsequent inhibition, are no real measure for stopping hair loss, they are a proxy for the efficacy of finasteride at best.

Your final dosing schedule should not be less than 1.4mg/week. To get close to the full benefits. It's ok to start off at less, and probably advisable as well. But ultimately, at least 1.4mg/week should be maintained. Studies show that 0.2mg per day was 80% as effective as 1 mg per day in increasing hair count, almost 5 times the dose. In addition, it was 64% as effective (this number should be closer to 75% based on the differences of medication period) for 25 times the dose at 5mg per day. Based on the pharmacodynamics and pharmacokinetics of finasteride, 0.5mg should be even more effective than 0.2mg, leaving it almost as effective as the 1mg dose, according to the logarithmic dose-response curve. Likewise, the EOD protocol seems to be just as effective as well, seeing as serum DHT levels do not begin to rise after the last dose of finasteride until at least 56 to 72 hours, consistent with the slow turnover for the human Type II enzyme complexes with a half-life ranging from 7 to 14 days.
Everyone has eventually heard how dangerous propecia is, we've all read horror stories on the internet on how finasteride gave me a limp dick, destroyed my sexual life and killed my dog. But the fact of the matter remains, unsatisfied people are usually the loudest. For every idiot on the internet creating threads crying about how Finasteride destroyed his life, there are hundreds of thousands popping the pill every morning and too busy to post their positive experiences on the internet due to living a good life with no stress or hair loss. The people with 'post-finasteride syndrome' are very sparse, and comprimise of about 100 people whom have originated the propeciahelp.com website. Naturally, their credibility should not be taken seriously, as they are nothing more than online reports. We do not know what doses they were taking, their source of medication, what kind of lifestyle they were running, what other medications they were on, what drugs they were doing, or their health state in general. In other words, there is no way to find out if you would personally tolerate it except to try, any side effects you may experience will most likely dissipate with time. If not, they will dissipate upon discontinuation, normally within one month at the most, since that is the timeframe required before making blood donations, and just enough time for complete turnover of 5-AR II enzymes.
Originally Posted by J Cutan Aesthet Surg. 2009 Jan-Jun; 2(1): 12–16. Several large population-based long-term placebo-controlled studies, using International Index of Erectile Function-5 questionnaire and objective method (Nocturnal Penile Tumescence) to assess the erectile function have demonstrated no clear evidence of the negative effect of finasteride on erectile function. Reduction in ejaculatory volume is the only established causal relationship between finasteride and sexual dysfunction. Though finasteride causes significant reduction in all the semen parameters except sperm morphology, they did not fall below the threshold levels to interfere with fertility. Therefore, the sexual adverse effects associated with finasteride should be viewed in relation to normal prevalence and natural history of erectile dysfunction in the population, age of the patient, other confounding factors and also nocebo effect.[1]
Originally Posted by Dermatology. 2004;209(2):117-25. n this comparative study of systemic finasteride and topical minoxidil, it was concluded that both drugs were effective and safe in the treatment of mild to severe AGA, although oral finasteride treatment was more effective (p < 0.05). Adverse events were not considered important either, and these side effects disappeared as soon as the treatment was stopped. [2]
Originally Posted by Dermatol Ther 2011; Jul-Aug;24(4):455-61. Finasteride, 1 mg daily administration on male androgenetic alopecia in different age groups: 10-year follow-up,” the Italian research team sought to fill a gap in our understanding of the long-term effects of treating hair loss with Propecia. The study tracked hair growth in 118 men between the ages of 20 and 61, with mild to moderate hair loss, who were treated with 1mg finasteride. These patients were evaluated before treatment and then again at 1, 2, 5, and 10 years on treatment. The authors concluded that a patient’s response to finasteride in the first year is a pretty good indicator of how effective long-term treatment will be for the patient. The better growth he experiences in his first year, the more likely he will have continued growth beyond 5 years of treatment. Among other findings, the age of a patient did have a statistically significant effect on the outcome, as patients older than 30 years had better hair growth in the long term. On the topic of side effects, 7 subjects (5.9%) experienced them, and some of those patients remained in the study because of what they perceived as the benefits of the treatment.
Originally Posted by JOU, Volume 174, Issue 3, September 2005 OBJECTIVES: To evaluate the incidence and resolution of sexual adverse experiences (AEs) in men with benign prostatic hyperplasia treated with finasteride 5 mg compared with placebo. METHODS:The Proscar Long-term Efficacy and Safety Study (PLESS) was a 4-year, randomized, double-blind, placebo-controlled trial assessing the efficacy and safety of finasteride 5 mg in 3040 men, aged 45 to 78 years, with symptomatic benign prostatic hyperplasia, enlarged prostates, and no evidence of prostate cancer. Patients completed a questionnaire at screening regarding their history of sexual dysfunction. During treatment, spontaneously self-reported sexual AEs were recorded. RESULTS: At screening, 46% of patients in each treatment group reported some history of sexual dysfunction. During year 1 of the study,15% of finasteride-treated patients and 7% of placebo-treated patients had sexual AEs that were considered drug related by the investigator (P <0.001). During years 2 to 4, no between-group difference was noted in the incidence of new sexual AEs (7% in each group). The drug-related sexual AE profile for finasteride was similar for men with or without a history of sexual dysfunction. Sexual AEs resolved while continuing therapy in 12% of finasteride patients and 19% of placebo patients. Only 4% of finasteride and 2% of placebo patients discontinued the study because of sexual AEs. In men who discontinued with a sexual AE, 50% and 41% experienced resolution of their sexual AE after discontinuing finasteride or placebo therapy, respectively. CONCLUSIONS: Compared with placebo, men treated with finasteride experienced new drug-related sexual AEs with an increased incidence only during the first year of therapy.
OBJECTIVES:To evaluate the safety and efficacy of finasteride 5 mg during a 10-year period in men with enlarged prostates. It is important that the long-term safety and efficacy of drugs intended for chronic administration in men with BPH be well understood. RESULTS: Twenty-four (56%) of the original 43 patients randomized to finasteride or placebo were judged as successfully treated during the 10-year finasteride follow-up (17 patients taking finasteride alone at 10 years and 7 patients who were taking finasteride alone when they discontinued during the 10-year follow-up for reasons not related to finasteride treatment). Altogether, 22 (51%) of the original 43 randomized patients continued finasteride treatment at 10 years (17 taking finasteride alone, 4 taking finasteride plus an alpha-blocker, and 1 taking finasteride for treatment of hematuria). Long-term finasteride treatment was well tolerated, with a low incidence of drug-related sexual adverse events occurring during the first year and even fewer occurrences during the 5-year open extension. No new adverse experiences occurring with increasing duration of exposure to the drug.
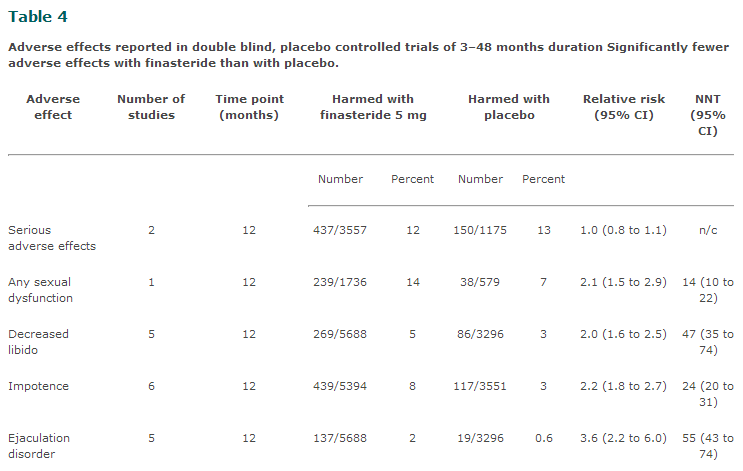
Note that most of these studies were done on old men with prostate problems taking 5 mg/day. A scientific deduction would entail that finasteride increases your risk for any type of sexual dysfunction by 2-folds compared to placebo. If you are prone to having sexual dysfunction, then finasteride might exacerbate the condition. If you are 40% likely to have ED, then that statistic jumps to 80%. If it's 0.1%, then your risk has increased to 0.2%.
2.3.1b Dutasteride
Dutasteride was shown to be more effective and showed less variation in inhibition of the different genotypes of 5-alpha reductase type II than finasteride. In a few genotypes, finasteride showed better inhibition than dutasteride, indicating that genotyping of patients would be beneficial when choosing treatment. This also provides a possible answer as to why some people who treat their hair loss with finasteride see a lot of improvement when they switch to dutasteride, and why a few instead notice a worsening of their condition. It may very well be due to some genotypes responding better to one drug than the other.
From a statistical standpoint, dutasteride is more likely to provide better results, but finasteride might be slightly more effective, despite the theoretically lower inhibition, this is why some people tend to stick to both. This is only statistically speaking, but I'd prefer to use science instead.
Dutasteride inhibits the same enzymes as finasteride, and even does a better job it on both the scalp and the prostate. With that said, any finasteride you ingest with dutasteride would be a waste. Seeing as Dutasteride effectively inhibits almost 95-99% of 5-AR2 enzymes with doses more than and including 0.5mg/day. Not to mention the 5 week half life of the chemical theoretically allows it stick around long enough to interact with any newly produced 5-AR enzymes around the clock. To put it simply, a 0.5mg dutasteride dose is comparable to 5mg of finasteride, so it would be like taking 6mg of finasteride, but a little better in the sense that dutasteride is a better target inhibitor of scalp tissue. Notice that 5mg of finasteride and 0.5mg of dutasteride had similar hair counts, and the effects will not be additive, at least not significantly to measure. While 1mg of finasteride (assuming that is your dose) did about 18% worse than both 5mg of F and 0.5mg of D.
Usually using both at the same time could be plausible if you intend to use a small dose of dutasteride coupled with finasteride. Some people take 0.5mg of dutasteride once or twice a week with 1mg of finasteride everyday, and experience some regrowth, even after as long as 4 years of finasteride use alone. But generally, you will not need finasteride at all at doses at and above 0.5mg/day of dutasteride, if anything, you could always increase the dose for even more effective results, albeit they should be marginal in terms of hair count.
Dutasteride has slightly more effects on sexual parameters than finasteride, but they fall within normal ranges nonetheless. Testosterone alone is sufficient to maintain qualitatively normal spermatogenesis in most normal men, the statistically significant parameters between dutasteride and finasteride in terms of sexual function would be the size of the prostate gland and volume of ejaculatory fluid. A higher risk of gyno or ED may also be prevalent as blocking 5-AR I would leave even more available free testosterone that could potentially be aromatized. But studies show that it is too insignificant to worry about.
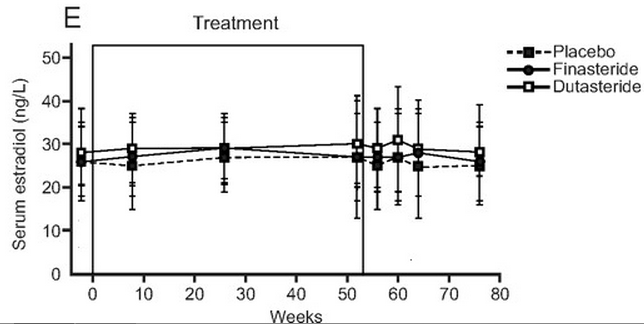
Dutasteride has a tolerability profile comparable to that of placebo when used daily for up to 2 years, with the exception of gynecomastia, impotence, and decreased libido, which occurred at slightly elevated incidences compared with the placebo group.
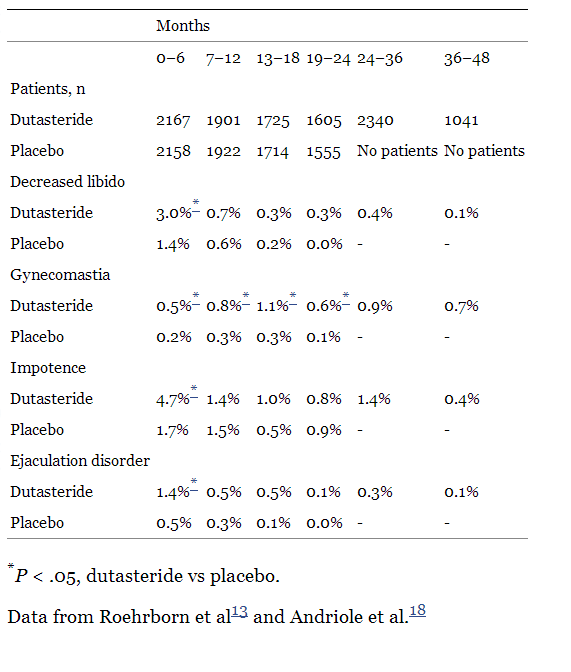
Interestingly enough, some studies show that Dutasteride actually has lower reports of side effects compared to finasteride, it is unknown why this occurs. While other studies show dutasteride with 1.5x the statistical probability of encountering side effects. The reason may be that there are a lot more studies done on finasteride, while very few done for dutasteride, so results might be statistically biased in that sense.
No long term studies has shown adverse reaction for dual 5-AR inhibitors, but then again, the longest study was almost for 4 years, excluding the one year follow up. Most medical literature at the moment tends to reflect it's safety profile, at least for the time being.
2.3.2 Minoxidil
Minoxidil does not stop baldness, it stimulates hair growth. It's a potassium channel opener and an antihypertensive vasodilator medication that promotes hair growth when used topically. It supposedly interferes with the beta-catenin pathway (check the chart on DHT pathways causing hair loss) and improves blood circulation, and therefore oxygen and nutrient delivery for hair follicles, resulting in speeding up the turnover of hair cycles on one end, and improving the follicles condition on another. On the other hand, 5-AR inhibitors stop hair loss, and your body may attempt to regenerate and reverse the miniaturization process which results in visible hair growth after a decent amount of time. When used synergistically, minoxidil is like steroids for these skinny weak hairs, and should give you results faster and better than when used alone.
Hair counts for minoxidil was slightly less than finasteride, their downside was it eventually loses it's efficacy under the effects of androgen damage, hair counts verrrry slowly begin to decline after a year of use, probably reaching baseline somewhere around 8-12 years. But with 5-AR inhibitors, that should no longer be a problem.
You should theoretically keep all the hair regrown using Minox, as long as you continue use. However, these will not be your 'real' hair, in the sense that once you discontinue, all the hair you were keeping alive using minox would die, and your true genetically predisposed scalp to hair loss will show. They say that minoxidil will not work effectively for 1/3 of people, maintain for 1/3, and regrow for the last 1/3. The 5% version is 45% more effective at regrowing hair than the 2% version, it also shows results much faster.
The foam version is a lot less messy and practical as a leave-on than the liquid form. Especially if you decide to leave the house. Also the liquid form has been known to cause irritations on the scalp. One of the main reasons the foam works better is because users are more compliant. The reason those who use the foam are more compliant is because the foam is easier to use. It is difficult to get the foam to your scalp if you have long hair but it can be done.
The liquid formulation contains propylene glycol, water, and alcohol. Propylene glycol is needed as a vehicle to solve minoxidil. However, most of the adverse reactions are related to hypersensitivity of propylene glycol. Itching, contact dermatitis and squamation of the scalp are attributed to propylene glycol content of topical minoxidil solution. With these aesthetic concerns, the topical foam of minoxidil was developed, which is propylene glycol-free. In the literature, there is no comparative study between the two formulations in humans. In an animal study, the foam formulation was found as effective as the liquid formulation. Once-daily 5% Minoxidil topical foam is noninferior and as effective for stimulating hair growth as twice-daily 2% topical solution in women with androgenetic alopecia and is associated with several aesthetic and practical advantages.
The official main side-effects of minoxidil may include pruritus, allergic dermatitis, palpitation, scalp irritation, and worsening of seborrheic dermatitis. If you are hypotensive in nature, then take caution. Dark circles and wrinkles have been reported as well, some studies show that minoxidil breaks down collagen in vitro, but that should not be problem as long as it isn't being systemically absorbed. I'm not sure how truthful that is, but it has been reported too many times on the internet to be ignored. I'd use foam only and keep it away from any direct skin contact on the face. Contrast to the finasteride scare, this may very well be overblown, either from improper use, or inexperienced observations.
2.3.3 Ketoconazole
Ketoconazole is a scalp exfoliator, and is commonly used to treat dandruff and oily hair. It is an anti-fungal steroid and has an anti-inflammatory effect. It most commonly reduces Malassezia colonization of the scalp, which has a hand in losing hair faster than normal through inflammation. if you are reading this, chances are you do have malassezia, it's more common than you might think. It also decrease sebaceous glands by about 20%, which may leave your hair a bit dry. Ketoconazole is used topically in the form of a 1% shampoo, 2% shampoo, or 2% cream. The 2% shampoo and cream are prescription grade, but you can easily get them from several online suppliers. The most popular brand is called Nizoral. The 1% shampoo can be found at your local pharmacy or bought online. By itself, ketoconazole isn't very effective, as it’s not powerful enough to stop the balding process, but I do think it is somewhat underrated; and when used in combination with the other two treatments listed above, it can certainly have a positive synergetic effect. There was even a study showing that 1% ketoconazole shampoo, used three to four times a week, can be as effective as 2% minoxidil. A 2% ketoconazole shampoo 2-3x/week should thicken up hair follicles nicely, since it tends to work better on hair follicle diameters than increasing their numbers. You don't need to use an additional shampoo as well. Just remember to use a good conditioner or hair oil, because it tends to dry the scalp. If your scalp becomes too dry or sensitive, drop down the usage, or buy the weaker version.
2.3.4 Spironolactone
Spironolactone is an anti-androgen that binds to and nullifies androgen receptors and thus competes with testosterone and DHT for it's place. Spironolactone, in it's oral form at least, is arguably the most powerful chemical in terms of treatment of hair loss, and every other androgenic function in the body. It is used mainly for male-to-female transgenders, although some individuals use it for treating hair loss. Spironolactone should not used in males because of the risk of feminization, so topicals are used instead. Like ketoconazole, topical spironolactone (also called “spiro/S5”) works by blocking androgens from attaching to the androgen receptors in the scalp. Also like ketoconazole, it is only marginally effective by itself, meaning it needs to be combined with other treatments to see any positive result.
The great thing about topical spiro is that it is metabolized in the skin and has very little, if any, systemic absorption, therefore it hardly ever results in side effects if used properly. Some users complain that it smells pretty bad, I do not think there is a way around this. Anecdotal evidence for the topical form is generally positive, although systemic absorption cannot be overruled. Side effects were reported, although no studies has been done to statistically measure the prevalence of it's side effects. A tip would be to not use it on a wet scalp, since moisture tends to increase absorption at a much higher rate through the skin. How fast and how much goes systemically is anyone's guess, this is nothing more than a precaution.
This effect is related to the binding of spironolactone with dihydrotestosterone receptors in the sebaceous glands. Our study demonstrates that 5% topical spironolactone cream acts as an antiandrogen in human sebaceous glands, competing with DHT receptors and producing a decrease of labelled DHT. At the concentrations used the effect has been only local. No side-effects were recorded.
The authors report their clinical experience with topical treatment of seborrheic acne with a 5% spironolactone cream in 20 patients, 11 males and 9 females aged 12 to 28 years (average 20.5). Treatment duration, about one month. Treatment proved remarkably effective in that it brought about complete regression of acne in 30%, improvement in 65% of the patients. The drug was always well tolerated, side effects were never observed.
Topical spironolactone 5% gel applied to the right cheeks of the subjects produced a significant reduction in the sebum secretion rates at 12 weeks
2.3.5 RU-58841
RU58841 is a non-steroidal anti-androgen that is used topically. In all honesty, not a lot is known about RU58841, other than it is a potent androgen receptor blocker whose clinical trials were discontinued (many believe strictly for financial reasons). There is not a lot of information about its safety profile. Normally, I would not include this drug in the list of effective treatments because it is an experimental, however there are enough users reporting positive results, there are very few reports of negative side effects, as RU58841 seems to get metabolized into an inactive compound once it goes systemic (inactive in terms of anti-androgenic effects anyway). Users claiming positive results say RU58841 performs just as well as finasteride but without the side effects, although there is no real hard data to prove this. Apparently, this is supposed to be the holy grail for topical anti-androgens as it is claimed to block almost all DHT on the scalp. Although it might be a hassle to get your hands on it, and prepare it for treatment use. Be advised, this is an experimental drug, so use at your own risk.
Here is a good guide on how to use it.
http://www.baldtruthtalk.com/showthread.php?t=12391
2.3.6 Tretinoin (Retin-A)
Tretinoin seems to help with the absorption of minoxidil, thereby increasing its effectiveness. That should be the case with all topicals as well. It may also have some mild regrowth properties on its own.
Topical all-trans-retinoic acid (tretinoin) alone and in combination with 0.5% minoxidil has been tested for the promotion of hair growth in 56 subjects with androgenetic alopecia. After 1 year, the combination of topical tretinoin with 0.5% minoxidil resulted in terminal hair regrowth in 66% of the subjects studied. Tretinoin was shown to stimulate some hair regrowth in approximately 58% of the subjects studied. One female subject with pronounced alopecia for more than 20 years had regrowth of hair using only tretinoin for a period of 18 months. Tretinoin has been shown to promote and regulate cell proliferation and differentiation in the epithelium and may promote vascular proliferation. These factors are important for hair growth promotion.
The efficacy and safety of combined 5% minoxidil and 0.01% tretinoin once-daily therapy appear to be equivalent to those of conventional 5% minoxidil twice-daily therapy for the treatment of AGA.
2.3.7 Derma Roller
Derma rolling is thought to initiate wound healing and thus triggering an embryonic state in the skin which made it receptive to receiving instructions from wnt proteins. The wnts are a network of proteins implicated in hair-follicle development. It should also help increase local absorption of topicals. The following study used 1.5mm needles once a week, and minoxidil was not applied until at least 24 hours after needling, twice a day everyday.
Results: (1) Hair counts – The mean change in hair count at week 12 was significantly greater for the Microneedling group compared to the Minoxidil group (91.4 vs 22.2 respectively). (2) Investigator evaluation – Forty patients in Microneedling group had +2 to +3 response on 7-point visual analogue scale, while none showed the same response in the Minoxidil group. (3) Patient evaluation – In the Microneedling group, 41 (82%) patients reported more than 50% improvement versus only 2 (4.5%) patients in the Minoxidil group. Unsatisfied patients to conventional therapy for AGA got good response with Microneedling treatment. Conclusion: Dermaroller along with Minoxidil treated group was statistically superior to Minoxidil treated group in promoting hair growth in men with AGA for all 3 primary efficacy measures of hair growth. Microneedling is a safe and a promising tool in hair stimulation and also is useful to treat hair loss refractory to Minoxidil therapy.
2.4 Non-chemical treatments
The topic of hair transplantation can be kind of tricky, so here’s what you need to know right off the bat.
-
A hair transplant involves taking the hair follicles from the back and sides of your head and “transplanting” them into areas of your scalp where you have lost hair. The reason this works is because the hair on the back and sides is usually DHT resistant and isn’t susceptible to androgenic hair loss.
-
Hair transplants have come a long way. They’ve gone from pluggy, doll hair looking results, to procedures where the final outcome is mostly undetectable if done by a talented hair transplant surgeon. HTs will most likely not look as good as a natural juvenile hairline.
-
There are two methods of hair transplantation. The “strip method” and FUE, or follicular unit extraction. The strip method involves removing a thin piece of scalp from the donor area on the back of the head. This is often called the “safe zone.” The hair follicles are then removed from this strip, divided up, and transplanted into areas of the scalp that are thinning or bald. The positive of this method is that it often produces great results, the negative is that many strip method patients are left with a scar on the back of their head, therefore they cannot wear their hair short or the scar will be revealed. FUE, on the other hand, is a newer technique, and involves using a specialized tool to take little “punches” of the donor area. These follicular units have anywhere from 1 to 4 hairs in them, and are then transplanted into the needed areas. Many patients opt for this method because it does not leave a linear scar, and they can still wear their hair short (some scarring can still occur in the form of little FUE dots. In my opinion, if this happens, they are still much less noticeable than a strip scar). In addition, FUE sometimes yields less of a result than the strip method. So it is up to the patient and his or her doctor to determine which method is the best.
-
Angle of insertion really matters, otherwise texture of transplanted hair is affected (ie some strands may point in a different direction significantly and look like a cowlick or something like that). Hair from the nape (base of back neck) is sometimes used to give the hairline a "softer" look, since hairs transplanted from the back look too thick and coarse. I'm still not sure how they transplant hairs on the temple so that they look natural. There are procedures like "dense packing" in which more hairs are transplanted at front to give an illusion of density.
-
There is not enough hair on the back and sides of your head to cover the entire top of your scalp. So if you are completely bald (Norwood 6-7) it is unlikely you will be able to get complete coverage unless you have exceptional donor density, which means you have way more hair on the back and sides of your head than the average person. This brings me to point #6.
-
You still have to take a medication like finasteride. If you don’t, you’re still going to lose the non-transplanted hair on the top of your head, and this may defeat the purpose of getting a hair transplant in the first place. So if you want full coverage, you must keep as much non-transplanted hair on your scalp as you can, as again, in most individuals there is not enough donor hair for complete coverage alone.
-
If you have a lot of body hair, you can transplant that to your scalp as well. The results (if done by a respected surgeon) are often better than you might expect.
-
Some people are not good hair transplant candidates because their hair loss is too severe or they have something called DUPA, which is diffuse unpatterned alopecia. This means that their “safe zone” is incredibly small, or that miniaturization is occurring on top of their scalp, in addition to the back and sides. This condition is much rarer than standard male pattern baldness.
-
Hair transplants are not cheap, especially if done by a respected doc. Even small procedures are going to cost a couple grand. As with most things, you get what you pay for. So if you go to a cheap doctor, you can probably expect cheap results. Therefore it is imperative that you do proper research on the hair loss clinic you select. Bottom line: Hair transplantation should only be attempted when medication fails to work, or hair loss has been stabilized. It’s also a poor idea for someone who is young (less than 25 years old) to get a transplant because you don’t know how far your AGA will progress. On the other hand, talented hair transplant surgeons can achieve miraculous results given the right circumstances. The key is research, research, research. In my option, the best transplant candidates are those who are Norwood 4s and under. If you are a Norwood 5 and beyond, getting complete coverage is going to be more difficult, however I have seen it happen, so all hope is not lost.
Wigs
Okay, let’s say you aren’t a good transplant candidate and medications were ineffective, what options are left? I’m not going to suggest a wig or hair system, as I know that sounds like a nightmare to a lot of people (me included). However, I will say there are some that provide amazing results like toppik, just throwing it out there.
Micro-Scalp Pigmentation
A couple years ago I would have said, “No, absolutely not.” But in recent years this technique has gotten increasingly better. It’s become a decent option for those that can rock the shaved look.Micro-scalp pigmentation is basically a tattoo on the scalp made to look like you just shaved your head and have “stubble” growing. Again, this is not a perfect science, but when you have run out of all other options, it is something to at least look into. It’s also not permanent, so you aren’t stuck with it if it looks bad. On the other hand, you will need touch ups every couple of years if it’s something you like. In addition, recent techniques involve micro-scalp pigmentation, followed by a small FUE procedure throughout the scalp to give an actual textured look. Do a quick search on this; you may be surprised at the results. This is an option for those that have severe hair loss, and who aren’t normal transplant candidates. Again, it’s not the best option, but an option nonetheless.
3. FAQ
Q: Im accepting the fact that I actually am receding. What is a good starter kit to get going on? A: The big 3, finasteride, minoxidil and ketoconazole. Or any combination of the former.
One hundred male patients with AGA of Hamilton grades II to IV were enrolled in an open, randomized, parallel-group study, designed to evaluate and compare the efficacy of oral finasteride (1 mg per day), topical 2% minoxidil solution and topical 2% ketoconazole shampoo alone and in combination. They were randomized into four groups. Group I (30 patients) was administered oral finasteride, Group II (36 patients) was given a combination of finasteride and topical minoxidil, Group III (24 patients) applied minoxidil alone and Group IV (10 patients) was administered finasteride with topical ketoconazole. Treatment efficacy was assessed on the basis of patient and physician assessment scores and global photographic review during the study period of one year. At the end of one year, hair growth was observed in all the groups with best results recorded with a combination of finasteride and minoxidil (Group II) followed by groups IV, I and III. Subjects receiving finasteride alone or in combination with minoxidil or ketoconazole showed statistically significant improvement (p<0.05) over minoxidil only recipients. No signifcant side-effects related to the drugs were observed. In conclusion, it is inferred that the therapeutic efficacy is enhanced by combining the two drugs acting on different aetiological aspects of AGA.
Q: I'm not sure which treatments I should use, what type of regime works best? A: This is their effectiveness in that order. 1- Dutasteride 2- Finasteride 3- RU 58841 4- Minoxidil 5% 5- Ketoconazole 2% / Minoxidil 2% 6- S5 cream
We still do not know for sure how effective RU and S5 are compared to the rest, we only know that they work. Ancedotal evidence claims that RU is even more effective than finasteride without the systemic effects, but this is speculative at best. A good line of treatment would be a combination of (1/2, 3/6, 4, 5). Most commonly, people use (2,4,5) with great results. I've yet to see a hair loss regime without (1,2) showing decent, sustainable progress. They are mandatory for the long term in my experience, if you want to stand any decent chance of keeping your hair at least seven years down the road, one of them should be used, I've seen people maintaining baseline or above for up to 15 years using 5-AR inhibitors.
Q: I'm 18 and reccedding.I'm worried that taking finasteride will inhibit any further facial growth as in development of facial bones or the mascularization of my features. Will taking fin not be a good idea considering my hormones are at their highest at my age? Would fin affect my growth? A: Sexual function in males fully develop before the age of 18 years old. The last thing that ends development at 23-25 is bone ossification, primarily the sternum and clavicles. The only things that keep growing with age are your nose, forehead, pelvis, prostate, and any other underlying cell tumors. Clinical trials for finasteride has been administered for men ages 18-70. Which suggests that there should be no problem in that sense. Furthermore, 5-αr II enzymes do not exist inside skeletal tissue, and since DHT is an autocrine hormone, which means that it only functions inside the tissue where it was produced, then it's absence from serum will not affect bones in any way. Long term studies on old men taking 5mg/day for BPH showed no change in BMD, which suggests that either only 5-αr I is responsible for maintaining bone density, or pre-existing testosterone and estrogen levels are sufficent.
5-αr II only exist in genital skin, testicles, prostate and hair, and they responsible for enhancing sexual development. Normally 21 seems like a safe margin. Prostate and genital growth most likely have ended at 18 years old. If hair loss is not aggressive, you could wait it out a few more years. Try other treatments like Ketoconazole, Minoxidil and S5 creams instead. The only effects that this might have in terms of masculinization is that the prostate will shrink about 20% in size and hair follicles will stop miniaturizing. Going by the model of pseudohermaphrodites, whom are people born with congenital deficiency in 5-αr II enzymes. The only difference between them and normal people past puberty is a slightly smaller prostate and a full head of hair, but are otherwise healthy individuals with regards to every vital sign.
Q: How do I know inhibiting 5-AR II enzymes will not harm me on the short or long run? Is there clear cut evidence for this? A: Going by the model of pseudohermaphrodites with absent 5-AR II enzymes. This is what their blood panel looks like (a) high normal to elevated levels of plasma T, (b) low normal to decreased levels of plasma DHT, (c) increased T to DHT ratio (d) normal metabolic clearance of T and DHT, (e) decreased levels of urinary 5α-reduced metabolites of C19 and C21 steroids, with increased 5β/5αurinary metabolite ratios, (f) decreased plasma and urinary 3α-androstanediol glucuronide, a major metabolite of DHT, (g) increased plasma levels of LH and/or FSH.
At puberty, these individuals undergo partial virilization of the external genitalia, although their secondary sexual hair remains sparse and they develop less male pattern baldness and acne despite normal sebum production. They undergo an increase in muscle mass, phallic growth, development of male body habitus, and deepening of the voice. Their libido is normal and they are capable of erections.
Q: I've read on forums that people do .25mg a day, .5 mg and 1mg a day, which is better for faster results? A: All doses possess almost the same efficacy. 5mg and 0.5mg every day will inhibit almost all 5-AR II enzymes, doeses and frequeny are highly irrelevant given the pharmacodynamics of the chemical. Consequently, results won't be faster regardless of the doses as well.
Q: What are the chances of it causing permanent impotence? A: Sperm mobility and morphology is regulated by testosterone levels, rats given 100mg/kg of finasteride showed no effect on fertility, so did humans with up to a single 400mg dose. Chances of finasteride causing impotence are close to zero. Chances of finasteride causing permanent impotence are statistically non-existent.
Q: So all the stories you read of it causing permanent impotence and/or loss of sex drive are bs? A: The pharmacodynamics of finasteride does not interfere with sperm mobility nor libido. The 1% you see reporting ED, low sex drives, impotence, gyno or any other related side effects are placebo. What this means is, 1-2% of the male population tends to exhibit sexual dysfunction, irregardless of finasteride. Finasteride seems to increase your risk for getting sexual adverse effects by almost 2-fold. According to most placebo controlled, and double-blind studies. With that said, if there was an 0.2% that you would get some form of Erectile Dysfunction at some point in your life given your genetic and health condition, then jumping on finasteride would statistically increase that chance to 0.4%. Even then the effects are temporary and dissipate with discontinuation.
Q: How about the transition from finasteride to dutasteride, what do you reckon in general? Can we use both at the same time? A: Using both together at the same time in not unheard of. Finasteride is a selective inhibitor of 5-αr Type II and III, while Dutasteride is a 5-αr inhibitor of all three types. But the thing is 5-αr I and III play no role in hair loss, so inhibiting them is unnecessary. But if this is true, then why does dutasteride grow more hair than finasteride if they both block the same enzyme responsible for MPB?
There are two reasons for this.
-
Dutasteride has a half life of 5 weeks, while finasteride has a half life of 6 hours, this means that there is a more steady-state concentration of the chemical in the blood at all times (not that this matters much).
-
Dutasteride, inhibits 5-αr II enzymes more effectively than finasteride on the scalp. IC50 for finasteride in prostate and scalp homogenates was reported to be 5.9 and 310 nM, respectively. What this means is, to get the 70-80% reduction of DHT in the scalp as it does in the prostate, you would need a dose of almost 50mg. On the other hand, 0.5mg of dutasteride had similar hair counts as 5mg of finasteride after 12 months. So it's nearly ten times as potent as finasteride for the scalp, but almost the same for the prostate. Dutasteride effectively blocks ~90% of serum DHT on 0.5mg/day, and up to 99% with 2.5mg/day. Side effects reported are generally higher than with dutasteride, and long term clinical trials have not yet been established for long term safety. With that in mind, the bio-locations of 5-αr I enzymes are present in vital organs such as liver, prostate, skin, bone, eyes and brain. DHT is normally an autocrine hormone, inhibiting them from tissue should not have serious consequences, but it may be uncomfortable with regards to physical and mental manifestations, should they arise.
Q: So, if the short half-life of finasteride is one of the reasons why it's less effective than DUT, why wouldnt we take it twice a day? A: Half life is a small part of the equation on why finasteride does not work as effectively. Finasteride is not only an inhibitor of 5-ar II enzymes, it's a suicide inhibitor. Meaning that once finasteride binds to a 5-ar enzyme, BOOM, it's gone. It forms an irreversible bond forever. So even though the half life of finasteride is only 6 hours, it takes up to a week for serum DHT levels to get to baseline after a single dose,

The reason for that is, the half life turnover rate of the 5-αr II enzyme is somewhere between 7 to 14 days. Generally, the amount of finasteride you take and the frequency in which you take it is generally irrelevant on a broad scale, seeing as it can be effective from doses as low as 0.12mg, and it takes probably at least 72 hours to have any appreciable change on serum DHT.
The bigger factor at work here is potency with respect to the scalp. Since the scalp has lower blood circulation than the prostate, it would naturally take a much higher concentration to give the same effects as it would for the prostate. IC50 for finasteride in prostate and scalp homogenates was reported to be 5.9 and 310 nM, respectively. So again, if you want the same effects that dutasteride on hair, you'd have to take at least 5mg/day, and up to 100mg/day to maximally inhibit scalp DHT, which is the main protagonist behind MPB. Seeing as it's obviously quite expensive to take that much finasteride per day, people just opt for Dutasteride doses ranging from 0.5mg to 2.5mg per day.
Increases of hair counts for both are as follows over a 24-week period:
Placebo -32.3 hairs Finasteride 5mg ~ 91 hairs Dutasteride 0.1 mg 78.5 hairs Dutasteride 0.5 mg 94.6 hairs Dutasteride 2.5 mg 109.6 hairs
Depending on you hair condition, see what fits you best. Obviously the best approach in terms of hair loss, is catching it early somewhere before a NW2 and use micro-doses of finasteride to maintain, to prevent ingesting a huge amount of chemicals.
Q: Will thick hair ever regrow in the temple areas or hairline if it is gone? A: Treatments should theoretically work on any scalp hair, but you need to understand that they mostly work to maintain existing terminal hairs, and may turn vellus hairs on the temples terminal depending on individual responsiveness. If that area is slick bald, chances are it's already gone. Treatments can only do so much, but it cannot bring back dead follicles most of the time, that's up to your body to decide whether it recovers or not. Finasteride increases hair counts by about 9% in the first year and 15% in the second year compared to placebo. While hair weight were greater 25.6% and 35.8%at 48 and 96 weeks, respectively. What this means is that finasteride does a better job on increased growth rate (length) and thickness of hairs than it does on increasing their number. To cut things short, the balder the spot you want to regrow, the less effective it will be. You'd have to get a hair growth stimulator as well, minoxidil is very powerful if applied consistently. I'd jump on the big 3. Finasteride, minoxidil and ketoconazole. These are the most studied and proven effective methods of hair treatments. Best results are not attained until at least 52 weeks with finasteride and up to 96 weeks, but earlier than that in other treatments.
Q: Does finasteride work on the front and hairline? A:
Originally Posted by J Am Acad Dermatol. 2012 Sep;67(3):379-86 Based on global photographic assessment, finasteride (1 mg) is able to increase hair growth in all areas of the scalp affected by male pattern hair loss.
Originally Posted by J Am Acad Dermatol. 1999 Jun;40(6 Pt 1):930-7 There was a significant increase in hair count in the frontal scalp of finasteride-treated patients (P < .001), as well as significant improvements in patient, investigator, and global photographic assessments. Efficacy was maintained or improved throughout the second year of the study. Finasteride was generally well tolerated.
Q: On Wikipedia it states that with a higher dosage of 5 mg 1 AND UP TO 10% experience erectile dysfunction. Is this a lie? A: Medical literature puts prevalence of side effects between 0.2% to 15%. In my experience with going through hundreds of journals and publication, the average seems to closer to 2% with placebo in mind. This is a recent Japanese study done in 2011 shows that the number is closer to 0.7%
Before now, there has been no study of finasteride use exceeding 1 year in Japanese men with androgenetic alopecia (AGA) except the study subsequently conducted from the development phase. Since the launch of finasteride, no study in a larger population had been reported. Ethnic variation of the onset age, progressive nature and degree of hair loss of androgenetic alopecia are known. The therapeutic effect of oral finasteride (Propecia) was examined on androgenetic alopecia of Japanese men. The efficacy and safety of finasteride (1 mg tablet) was evaluated in Japanese men with AGA in the long term. The study enrolled 3177 men given finasteride 1 mg/day from January 2006 to June 2009 at our clinic. Efficacy was evaluated in 2561 men by the modified global photographic assessment; the photographs were assessed using the standardized 7-point rating scale. Safety data were assessed by interviews and laboratory tests in all men enrolled in the study. The overall effect of hair growth was seen in 2230 of 2561 men (87.1%), in whom hair greatly (11.1%), moderately (36.5%) and slightly (39.5%) increased. The response rate improved with increasing duration of treatment. Adverse reactions occurred in 0.7% (23/3177) of men; seven men discontinued treatment based on risk-benefit considerations. No specific safety problems associated with long-term use were observed. This study represents data collected at a single institution. Many patients did not receive follow-up examination. In Japanese men with AGA, oral finasteride used in the long-term study maintained progressive hair regrowth without recognized side-effect.
Q: Will treatments possibly regrow what I have lost and help me to get a NW1? Did my balding stop? A: Possible? Yes. Probable? unlikely. Once a hair follicle miniaturizes to the point where it cannot penetrate the skin anymore (bald areas), chances are the follicle is past recovery most of the time. This is especially true for mid-anterior regions of the scalp, including the hair line and temples obviously. Normally, when the triangle shaped hair above the side burns is gone, it's actually a good sign. Let me explain why. That part of the scalp is usually more resistant to androgens and tissue expression for hair loss than other vulnerable parts such as the hair line, some of the crown, and temples. So in essence, by losing that part, it's actually an indicator that most, if not all of your hair loss has already happened! Keep in mind that this not a rule, and exceptions do exist.
Q: Why choose finasteride over dutasteride? A: The effectiveness of finasteride compared to dutasteride is not immense in magnitude. Comparing extremes, it seems that as little as 0.2mg/day of finasteride grew 61 hairs compared to a whooping 2.5mg of dutasteride growing 109 hairs. A more realistic dose for both would be 1mg/day for F and 0.5mg/day for D, with hair counts 77 and 94 respectively. As you can see, dutasteride did only 18% better than finasteride on hair counts, while inhibiting serum DHT a lot more from taking out 5-ar type I enzymes as well.
Q: Does Finasteride effect muscle building and body fat? And does it cause face bloating? A: Finasteride does not have any effect on muscle building. DHT is neither androgenic nor anabolic towards muscle tissue. It gets deactivated once it reaches muscle tissue by 3-alpha hydroxysteroid reductase enzyme. Testosterone is the only anabolic hormone in the blood, although seeing as DHT does have some role in CNS function, it is normal to notice a slight decrease in explosive strength and contractile power when it is reduced, but no effect otherwise on cross-sectional muscular hypertrophy. If anything, the slight increases in free testosterone provides a more anabolic environment for muscle tissue. Facial bloating is a side effect reported, it mostly happens when E2 levels rise which allows for more water retention to occur. If you are lean to begin with, then there will be less propensity for adipose tissue to accumulate intracellular fluids.
Q: What about Finasteride's effects on the central nervous system? There is recent evidence suggesting that 5-alpha-reductase inhibitors may inhibit neurogenesis in the hippocampus (impairing memory) and may also reduce levels of particular neurosteroids, such as allopregnanolone. A: While 5-alpha-reductase can influence progesterone, corticosteroid and androgen metabolism, the current therapeutic role for finasteride in humans involves blocking the conversion of testosterone into DHT, the major androgen metabolite. However, potential effects of inhibition of progesterone metabolism in the CNS could theoretically be present. Finasteride crosses the blood-brain barrier, and thus can be used to inhibit 5-ar activity in the CNS.
Numerous studies have documented that systemic administration of allopregnanolone produces anxiolytic and antidepressant effects. A study involving rats showed that finasteride injected into the amygdala increased the bouts of anxiety and depression. However, it has been suggested that the the extent or rate of change in allopregnanolone was the bigger factor in experiencing anxiety and depression. Also, all subjects experiencing these cognitive side effects also had a history of depression, anxiety and mental illness. A subsequent study of quality of life (but not depression explicitly) in men taking finasteride also failed to provide evidence that finasteride detracted from life quality. In a double-blind, placebo-controlled study there was little or no difference between placebo and finasteride groups in ratings of general health and life satisfaction. Animal research has yielded a promising body of evidence that supports the role of finasteride being a depressogenic drug, while clinical trials on humans showed mixed results.
Another consideration is that neuroactive steroid effects may be more pronounced in experimental animals than in humans, a finding that is not unique to allopregnanolone. For example administering DHEA to animals showed an improvement in memory, while the opposite in humans. Judging by the levels of neurosteroids, it seems that finasteride does slightly lower these levels, but they still remain within normal ranges. Keep in mind that finasteride only inhibits 5-AR II & III and leaves type I generally intact, which still leaves plenty of 5-AR for the brain to maintain normal function. What's really important is not the levels of neurosteroids in the brain, it's the rate of change that causes the bigger effect, whether positive or negative. You will likely feel normal again after some time either on medication, or off it.
With that said, the slight reductions of neurosteroids should still leave you happier overall due to maintaining your hair, and having an overall better quality of life. Personally, being bald would leave me extremely depressed and anxious. Weigh the pros and cons yourself.
Q: I'm 3 months in using treatments and my hair has never been worse. Should I wait it out, hop off, or what? A: Shedding up to 100 hairs a day is normal. You have about 110,000 hairs on your scalp on average. Assuming hair doesn't grow back, this means that you need to shed 100 hairs everyday for 3 years, to go completely bald. Shedding hair more than that is also expected on hair loss treatments. How can new hair to grow out stronger than before if there is another follicle in it's place? Shedding usually means new hair are pushing the old ones out, and that it's working. DHT miniaturizes and sheds hair very progressively, you will not lose a significant amount of hair in only a few months, so it's probably only the treatments working.
What happens with most treatments is this. The follicles must regress, shed the old fiber, rearrange themselves into a bigger hair follicle, and start making a new, improved fiber. This would inevitably lead to a temporary shed phase. You're seeing your hairs respond. Its unfortunate that the first sign of new hair growth is seeming hair LOSS, but that's the way it works, quite often. There is a belief among some dermatologists that an initial shed phase when first starting to use a treatment for hair loss is inevitable regardless of the treatment used. Because of the hair follicle's inflexibility in changing the nature of hair growth mid stream.
For any drug to promote hair growth it must involve hair follicles entering telogen to rearrange themselves into a larger follicle under the influence of the drug. I suggest you form a specific hair regimen and stick to it. Changing doses or frequency might trigger new hair shed cycles. Finasteride and dutasteride especially take a significantly long time to realize the full benefits. In laymen terms, this is because you tend to block all DHT molecules that was bound to the hair follicles, thus hair needs to start repairing and regrowing after taking a new breath of fresh air, which should last a couple of hair cycles to see the final results. Although significant regrowth is not a rule, depending on the severity of hair tissue expression to damage, especially in the temporal region. Experiencing second or third shedding phases is expected as well.
Hair counts: Finasteride treatment produced progressive increase in hair counts at 3, 6, 9 and 12 months [Table - 3], whereas the placebo treated patients continued to lose hairs at 6, 9 and 12 months (all p values, <0.05 vis a vis baseline). At month 12, the study demonstrated an increase of 20.56±4.73 hairs (mean±SE) for finasteride and decrease of 9.56±5.53 hairs for placebo, with a net difference of 30.12±7.31 hairs between the two groups. At month 12, 87.5% of the patients treated with placebo had decreased hair counts in comparison to only 21.74% of the patients treated with finasteride. Thus, finasteride was significantly superior to placebo in increasing the hair counts, the improvement starting as early as 3 months.
-
Appearance of hair: Finasteride treated patients had statistically significant superior rating at 6,9 and 12 months (p value, <0.05) but at 3 months, the difference between the two groups was not statistically significant (p value, >0.05).
-
Hair fall: Finasteride treated patients were significantly better rated at each point of follow-up (all p values, < 0.05).
-
Hair growth: Finasteride treated patients had significantly better hair growth at 6, 9 and 12 months (p value, <0.05); however the difference in rating between the two groups was not statistically significant at 3 months (p value, >0.05).
-
Bald areas: Reduction of the bald areas in finasteride treated patients was rated as significantly better at 6 and 12 months (p value, <0.05) while at 9 months, the response to the drug was not significantly superior to placebo. At 3 months, placebo was rated superior to finasteride, however it was not statistically significant. At 12 months, the percentage of patients assessing themselves as improved for hair appearance were 60.86% in finasteride group and 18.75% in the placebo group. For hair fall, it was 73.9 1% versus 43.75%, for hair growth, it was 52.17% versus 12.5% and for bald area, it was 39.13% versus 18.75%, in the finasteride and placebo groups, respectively.
d) Clinical assessment: The clinical assessment of hair growth also revealed that finasteride was superior to placebo. The finasteride treated patients were rated superior to placebo at each point of follow-up, but it was significant only at 6, 9 and 12 months (p value, <0.05). At 12 months, 56.52% of patients in the finasteride group were assessed as improved, whereas in the placebo group only 18.75% were rated as improved.
Q: How effective do you believe finasteride is when you have genetically inferior hair. In other words, if you were meant to bald can finasteride stop this process. What percentage of treatments are successful. And if you really are meant to be NW5 or some crazy sht because your hairs are sensitive to DHT, does that mean even finasteride cant save your sorry ass as it cant reduce the levels of DHT enough for your ing sensitive hair to stay on your now bald head. Also do you believe that DHT is an unknown subject and that reducing its natural amount can have adverse consequences down the road that we are not aware of? After all finasteride as I understand is relatively new. A: At the VERY least, it will hinder the loss significantly, and you will get to the norwood scale that your genetics intended to at a much later stage in life (hopefully). Some people just don't respond to treatments, whether that stems from poor bio-location distributions of 5-AR I and II enzymes, reflex hyperandrogenicity from medication, low IGF-1 levels which proved to provide people with worse results than placebo, or simply hair loss that is just too aggressive to be controlled. But for these people, hair is probably going to be the least of their worries. The most powerful treatments are 5-AR enzyme inhibitors by far. Not taking into account oral anti-androgens, as these should not even be an option.
DHT is not an unknown subject. Finasteride for hairloss was not an "accidental discovery". Finasteride has been around and studied on humans from as far back as the 1980s. It's clinical efficacy and safety profile is extremely well documented. We have 7 year clinical trials for finasteride for benign prostatic hyperplasia with 19,000 subjects in which 17,000 of them completed. Cases for long term side effects after the study's follow up conclusion have been reported to be zero controlled with placebo. Some trials even earlier than that had subjects take as much as 70 mg/day, with no side effects reported after discontinuation, yet we have people on the internet crying that their dicks fell off after 3 pills of propecia. While we have lots men on finasteride for over 15 years with nothing to report. DHT's function is well established and thoroughly studied in human and animal models. The prostate produces more than half of a male's DHT. Old men going through prostatectomy, which means almost all of your DHT in sexual organs goes out the window, are still able to achieve erections a month after surgery, although no ejaculation fluid is present on orgasm, clearly.
Q: Decreased ejaculation volume and weaker orgasms might be legit sides to consider when increasing finasteride doses or switching to dut then? What other side effects can I expect? A: Decreased ejaculatory volume is expected on both treatments, but obviously with varying degrees. Finasteride can maximally decrease prostatic size by ~20-25%, and almost the same for ejaculatory volume. I believe Dutasteride does this even more powerfully. Orgasms and libido are mental more than anything, your brain has control over that. But for a healthy male capable of normal levels of testosterone, it's enough to maintain prostatic mass and prevent cell apoptosis (death), and maintain a healthy libido and orgasms. This was proven in castrated rats supplemented with exogenous testosterone alone and DHT alone. Note that both testosterone and DHT serve the exact same functions in humans, but one in a more potent form. This is why serum testosterone levels tend to increase after medication, as compensation. Pseudohermaphrodites also have average T levels close to 800 ng/dl, when the normal range is 350-1100. The second most common side effect is a dull testicular ache. The testicular pain from finasteride is induced from a mechanism parallel to secondary hypogonadism, where LH levels tend to drop after an increase in sex steroid concentrations. This usually gives testicular ache in the first month or so, until the body maintains homeostasis. But that only happens to a minority of users from what I've seen, I've personally experienced it however.
Q: You have to be off fin if you want to get your wife pregnant? fin actually affects fetus development? A: You do not have to be off of fin to get your wife pregnant, finasteride does not affect sperm counts immensely. Finasteride, even at low doses, may cause reduced sperm counts in some men, it would be wise to discontinue use in subfertile men with oligospermia, until pregnancy is achieved. As for pregnancies, it is usually advised to keep finasteride tablets away from pregnant women, but not women in general. Seeing as there exists a possibility that powder might get inhaled or absorbed through the skin, and affecting fetal development. In the event that it happens, the fetus WILL develop into a pseudohermaphrodite, where a potential boy would be raised wrongly as a girl, resulting from the severe under-development of genitals and secondary-sex characterisitics. Finasteride getting transferred through semen is negligible and almost 100 times less than the least effective serum concentration quantities.
Q: What finasteride doses should I use? A: Generally, 1 mg per day is almost 25% more effective than 0.2mg per day in terms of hair counts, although there is a very steep diminishing margin of returns as you increase doses, it still exists. I'd generally say 0.5-0.625mg is an optimal cost-benefit dose, since it's likely only 5% less effective than 1 mg per day, but at half the cost.
Q: When doctors prescribe propecia, those come in 1mg tablets that you take EVERYDAY. You think it might be too much for the body and therefore leading to all these undesirable side effects? A: I do not think dose is highly correlated with side effects, although it tends to exist. For example, 5 mg/day decreased prostatic mass more than 1 mg/day did in 6 months, although they are virtually similar in effectiveness. This leads me to believe that higher doses would only increase risks of complications in people prone to having side effects. If you were going to have side effects at 300 mg/day, chances are you'd still have them at almost any other dose. Early clinical trials for finasteride had subjects ingest up to 100mg/day for a week with no reported side effects after discontinuation, while about 2-5% experienced side effects during the study.
In essence, the blood concentration of finasteride means little, since a dose of 1 mg produces just about the same result during peak concentrations after a single dose as 100 mg. The only advantage a 100 mg dose has is a more sustained concentration of finasteride in the blood, which would take about 60 hours for it's serum concentration to reach the same levels that 1mg would in 24 hours. For obvious reasons, this is not a cost effective method for medication. Furthermore, blood concentrations of finasteride reach a steady state after everyday dosing in about 4 days, where the peak concentration does not increase any further. This is true for any dose. For example, taking 100mg/day would give you a maximum peak concentration levels comparable to a single dose of 106.6mg, assuming chemical half-life metabolization is 6 hours. For 1mg/day it's 1.06mg, for 0.5mg/day it's 0.533. What this means is, as long as you manage to take doses at least right on half-life (every 6 hours), and not before that, then the maximum potential for serum concentrations of finasteride is double that dose.

You can see the drop is exponential as by nature of the 6 hours half life. No accumulation of finasteride occurs as a result. Generally, the amount of finasteride you take and the frequency in which you take it is generally irrelevant on a broad scale. Seeing as it can be effective from doses as low as 0.12mg, and the fact that it's a suicide inhibitor, which takes 5αr-II enzymes some time to regenerate, probably at least 72 hours to have any appreciable change on serum DHT, given the half life turnover of 5αr-II has been suggested to be anywhere from 7 to 14 days. Although tissue DHT concentrations which is the more important principle here, can be sooner than this. With that said, I'm guessing either a big dose every 72 hours with at least 1.25mg or 0.5-1mg EOD or 0.25-0.5 ED should all give results that are quite similar, and almost as effective as the most optimal doses.
Q: How long should it take for Dutasteride to "kick in" or "reach blood plasma levels" or however you say it? If I was going to get sides, how early could I expect them? A: Following daily dosing, dutasteride serum concentrations achieve 65% of steady-state concentration after 1 month and approximately 90% after 3 months. In volunteer studies of Avodart, single daily doses of dutasteride up to 40 mg/day (80 times the therapeutic dose) have been administered for 7 days without significant safety concerns. In clinical studies, doses of 5mg daily have been administered to subjects for 6 months with no additional adverse effects to those seen at therapeutic doses of 0.5 mg.

Doses at or larger than 0.5mg/day achieve a 95% of steady state over 112 days. (70%, 90%, 95%). However, the blood concentrations say little. Their effects on serum concentrations of DHT, and thus inhibition of 5-AR enzymes is much faster. Typically within 1-2 weeks. Side effects should be obvious, and strongest at the beginning, concurrent with 5-AR inhibition. If they go away with time, then you are most likely fine.
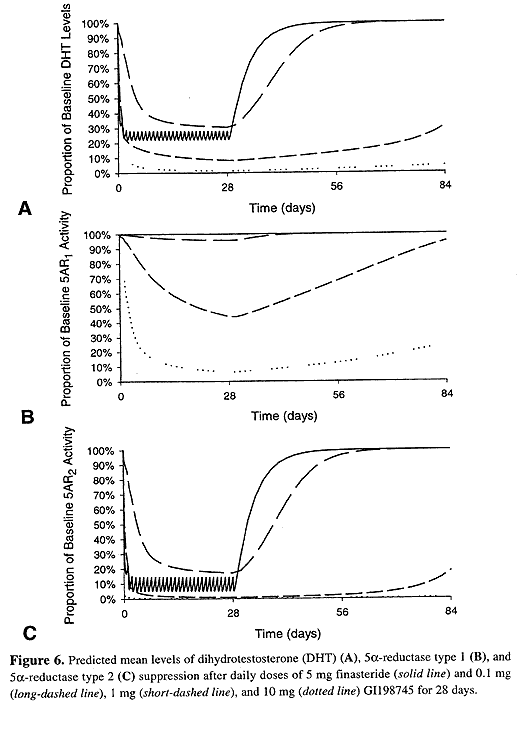
GI198745 is dutasteride.
Q: I'm getting proscar this week, how do I cut the pills to 0.5mg? A: You have two options, either cut them evenly using a pill cutter or a sharp knife. Then cut each fifth into halves. You obviously won't get it exactly the same, but that should not matter, finasteride is effective at almost all doses. Or dissolve them in an alcohol (vodka works fine) solution and titrate doses.
Q: Those who are prone to estrogenic sides, how to prevent the conversion of testosterone to estrogen? A: I can outline some natural ways to avoid build up of estrogen.
-
Aromatase enzymes in the male body is synthesized in adipose tissue, adrenal glands and testis. But only about 25% is aromatized in the gonads and adrenal glands, the rest comes from fat. So losing weight, especially around the midsection will limit estrogen conversion.
-
Cut down on alcohol and drugs, drinking excessively can increase the body's conversion of testosterone into estrogen, especially in fat cells. It can also block the liver from effectively eliminating excess estrogen. The use of anabolic steroids, marijuana, cocaine and other drugs can affect hormone levels.
-
Supplement with zinc, and eat lots of vegetables and citrus fruits, especially broccoli, they inhibit aromatisation. Zinc is also food for the prostate, which you will be needing.
-
Exercise and do cardio regularly. Research shows that physical activity curtails overproduction of estrogen.
Q: Can I check blood levels for DHT to see if I'm prone to AGA? A: Serum DHT levels mean little in terms of hair loss. In fact, subjects with high serum levels of both Testosterone and DHT show less balding than the opposite. The correlation is a negative one. Blood serum DHT was actually higher in non-balding men. High serum DHT = lower chance of alopecia, but high local 5-AR activity = hair loss. The overall increase in both aromatization and 5-AR activity with age, as well as the tissue specific expression of those enzymes thusly explains why men begin losing their hair as they get older, although their total androgen levels begin to decline.
Q: Why do we have DHT? does life hate us? A: I'll try to explain this in simple English.
Testosterone is the mother of all hormones in humans and animals. It is the main hormone responsible for all anabolic and androgenic functions in the body, including developments in the brain, bones, organs, skin and hair. It's testosterone that shapes your brain during development to carve out pathways for the behavioural aggressiveness and masculinity of the male gender. It grows your bones, muscles, vocal chords, facial hair, body hair, penis, and prostate during puberty, and maintains them post-puberty. They are mostly produced from the gonads, where they provide most of your body's supply.
So what advantage does DHT have over T? Well, DHT is merely a derivative of T, an upgrade. It is the more powerful and more advanced version of testosterone, although they serve exactly the same functions when bound to androgen receptors, the only upper hand T has to DHT is that it is anabolic towards muscle tissue, while DHT is not. But if T can do everything DHT can, why do we need it? Again, it is simply an 'upgrade' your body has provided in case testosterone levels drops too low, or there is simply not enough free testosterone to maintain all of the androgenic functions the body needs. As mentioned, poor T is working all alone, even if it is present in very large amounts compared to DHT. So just to be safe, the body produces 5-AR enzymes. We have numbered them Type I and II because this was the order in which we have discovered them. Type I is present mostly on organs and skin. While II is present mostly on hair, prostate, genitals and seminal vesicles. It is T's sidekick and makes sure that all these organs are getting a constant flow of androgens in case T gets tired from doing all the work. DHT is 3 times stronger than T in the sense that it has 3 times more affinity to receptors, so it can potentially hold on for 3 times longer.
Another advantage that DHT has is that it does not have to brainlessly flow around the body looking for empty ARs to bind to, it is produced locally at the organ which needs it. For example, since the prostate is such an androgen intensive gland, it has large amounts of 5-ar II enzymes to give it all the hamburgers it needs to keep fat and chubby, Because T has other things to do other than hang out next to the prostate. DHT also has another advantage over T, it cannot be converted to estrogen. So no matter how much DHT the body has, it cannot be aromatized, and thus can be produced safely at any quantities (until MPB and prostatic hyperplasia), unlike free T which can be aromatized. So actually, DHT is not bad at all. It's just that sometimes it's androgenic power is too strong for people with sensitive hair like most of us, so we need to kick it down a notch to delay the process.
Q: What can you tell me about biotin? And what other supplements do you recommend for healthy hair? A: There are lots of vitamins and minerals playing part in skin, hair and nail growth. However, as long as you are not deficient in any of them, then overdosing would actually do very little.
Common ones include:
- Niacin
- Biotin
- Vitamin D
- Vitamin C
- Zinc
- Omega 3 FAs
- Magnesium
- Iron
- Selenium
Q: I have reason to believe scalp inflammation, and acne plays a role in hair loss. Could you further elaborate on this? A: Yes, sebum overproduction in the scalp has been linked to hair loss, especially androgenic hair loss. Sebum keeps hair and skin supple. This is the type of oil that your skin produces from sebaceous glands. These glands hypertrophy and enlarge during puberty from increased testosterone, when the free flowing testosterone molecules bind to the 5-AR1 enzymes on the skin, it gets reduced to DHT, which increases activity of these glands to produce sebum (oil). The theory behind it's role in hair loss is this:
-
It blocks oxygen and nutrients on the scalp from reaching hair follicles, by coating the follicles exterior under the skin and on top.
-
Overactive sebaceous glands are a precursor to high DHT reduction. So if you have high 5-AR1 reductase activity (which is the leading cause for acne), then you probably have high 5-AR2 activity as well, which is directly to AGA as explained before.
-
The sebum is a perfect environment for bacteria and fungi to grow. Your immunity system senses this as foreign protein from outside of the body, and attacks the scalp and hair follicles to prevent 'contamination'. This biological response traps blood on the scalp and causes inflamed scalps, itching, and most probably hair loss as well.
Q: What's the reasoning behind one temple receding more compared to the other side? A: Different bio-locations of 5-AR enzymes and different androgen receptor sensitivities on the hair follicles in both sides. We do know that symmetry is very rare in nature, this must be no different. It's nothing more than a statistic, but 70% of people seem to recede at the right temple before the left one. Probably genetics, and if it is, then this statistic would only grow larger.
Q: Does creatine cause hair loss? A: Short answer, no. Long answer, Nope. Creatine might indirectly increase the release of free testosterone through higher workout volumes than placebo, which might increase DHT conversion on scalp tissue. But it has no other effects on hair otherwise.
Q: We've been hearing about cures to AGA for the past few years by cloning hairs? Are we getting close to something significant? How long do we have to wait? A: The truth is that we are closer to walk on the face of mars than cloning hairs, cloning is not even close to happening, the media gives too bright futures on that. It is really hard to say when cloning hairs will be a retail, but it surely is not going to happen until at least a decade. The permits for cloning itself is going to take another couple of years.
Nothing outstanding as of yet, and not anytime soon. A big part of the equation is profits. Not to mention the amount of R&D to produce an affordable retail cure will be very expensive and lengthy, and only likely possible by big pharmaceutical companies, whom have no incentive to discontinue their lines of products for temporary hair treatments. No one is interested in funding a research and development team to create a retail cure, the big pharmaceutical companies are all collusive and make much more operating profits selling temporary hair treatments that keeps them a going concern. While the smaller pharms do not have the capital that the big pharms have to fund such a project. Having said that, since stem cell research, follicular cloning and genetic engineering is not realistic anytime soon, the only "cure" I can think of some kind topical intervention to disable the protein gene responsible for hair loss, but that could be very complicated and would take years until trials are released for long term safety and efficacy. Finasteride, minoxidil, topical anti-androgens, and hair transplants are the best we've got so far, and most likely will stay that way for a long time to come, so make use of them.
Q: HELP ME !!! I NEED YOU TO TELL ME HOW TO INTEGRATE ALL THESE TOPICALS INTO A WORKING REGIMEN? RETIN-A, MINOX, S5 CREAM etc etc. I'M BEGGING YOU! I'M SHEDDING LIKE NO TOMORROW LATELY A: Retin A, wait 15 minutes, Minoxidil, wait 30 minutes, S5 cream. AM and/or PM except Retin-A only once a day or every other day. On areas where hair is thin.
Q: Where can I buy treatments? A: Finasteride, Dutasteride and Ketoconazole 2% are prescription only, you'd have to ask your local dermatologist. You could still order them online however in the following link
http://www.inhousepharmacy.biz/
Fincar, proscar, avodart and dutas are all fine. Minoxidil should be available in a drugstore near you.
S5 creams should be sold here:
www.hairlosstalk.com/shop/s5-cream.html
There is no real difference between the day and night versions. Just get the day cream.
Q: What do you personally use? A: I've started with 0.25mg of finasteride 3x/week last June, bumped up the dose a couple of times, and ending up with 0.5mg ED since late October, I also use a generic ketoconazole 2% shampoo whenever I shower. Supplements I use on the side are 25 mg of elemental Zinc, Vitamin C 1g/d, Vitamin D 200,000 IU/m and Creatine 5g/d.
Q: I don't even know why people bother with this crap. Who wants to apply foam to their head twice a day or take medication everyday for the rest of your life? I would feel more confident being bald rather than taking medication to keep hair on my head. All it shows is insecurity which would make me feel even more insecure, almost because I'm living a lie. A: Taking medication to maintain appearance may not stem from insecurity, and if anything, an insecure person trying to keep his hair using treatments will be even more insecure going bald. We do it purely for cosmetic reasons. Call it vanity if you wish, but I have no problems taking a pill every day, rather than constantly worry about how much has my hairline receded and how much time I have left to enjoy what remains. Do what makes you happy, and to each his own.
Q: I was tired of being insecure about my receding hairline so I decided to cut it, sort of regretting it now because I'm getting a lot less female attention its still better then worrying about it and checking the mirror every few minutes. While I agree it's unnecessary for people to come in here and say just shave your head, it's not really accurate to say women hate bald men. Most women might prefer men with hair, but that doesn't mean they hate those without hair. There are many women who have expressed their attraction for bald men such as Jason Statham and Johnny Sins. Of course, not everyone has the facial aesthetics to pull off the shaved head look. A: Confidence goes much further than looks. All women prefer men with hair, it's not a deal breaker, but you will have to lower your standards in most cases, unless you have something else to compensate for outside of the looks department (which you should). Jason Statham is not an accurate representation, he has a smoking hot model girlfriend, but he is also rich and famous. I sincerely think women would not do double takes on him in public if he wasn't a celebrity. But to be honest, you shouldn't be doing this for women, plenty of married men still try to keep their hair. For some, it's a big part of their identity, and the person they are trying to represent to society.